Podcast: Play in new window | Download
Episode 8: How childhood neurodevelopment turns into road rage, or becomes rewired completely. You decide. (This one will save loss, pain, and lives.)
Intermittent Explosive Disorder (IED) is an official diagnosis for an anger control problem. It is characterized by impulsive, unexpected anger and aggression that is disproportionate to the situation. The diagnosis code is F63.81 in the International Classification of Diseases, Tenth Revision. From the outside, the world sees an angry person, but they are often riddled with guilt about their behavior. If unable to modify the personality and self-care to accommodate for IED, these people burn all their bridges and wind up totally alone. They need to Mindshift.
Download the Ambassador Slides HANDOUT to share.
Trileptal and My 2-Minute Speech
- “When a threat is perceived, adrenaline triggers an uncontrollable reaction.
- Intermittent explosive disorder is a hard-wired anger reaction, almost always originating from PTSD. This is why traditional cognitive approaches to anger management are often inadequate.
- It is exactly the opposite of a trained operator or martial artist. However, if the brain is exposed to enough toxicity, a veteran will slowly lose their brain’s ability to inhibit.
- A mood-stabilizer is a “10 second fuse”. It will let you notice the feeling without impulsively acting on it.
- Walk away from the anger-provoking situation the first 5 times you get mad, so you can learn how the medication will help you go calm yourself down. Then, practice talking through your problems knowing you can now walk away if you need to, so eventually you won’t have to live in fear of your anger or be made to feel like a doormat.”
Trying to overcome IED without help is like dancing stoned on the edge of cliff. By definition, not taking life-threatening behavior seriously is absolutely the most irresponsible decision for mental health. Afterall, mental health equals self-care.
Why won’t this work on children?
From the outside, children and adults look the same emotionally with temper tantrums. The adult with IED, however, is overreacting in anger despite a previous decision to keep anger under control. Children haven’t yet made decisions on the kind of person they want to be (superego), they are running into a nonstop series of life lessons and reflexively react based upon their hardwired subconscious programming. It’s not the kid’s fault. By that same logic, it’s also technically not the adult’s “fault”, but it is their responsibility. Adults in the heat-of-the-moment react violently without a conscious choice – the prefrontal cortex is not involved in a decision until after the action has begun. Trying to stop yourself once your anger has progressed to screaming and violence is literally trying to overcome all of your life’s pains and griefs that have come to bear, and in the most dangerous and unhealthy way possible. You need to Mindshift.
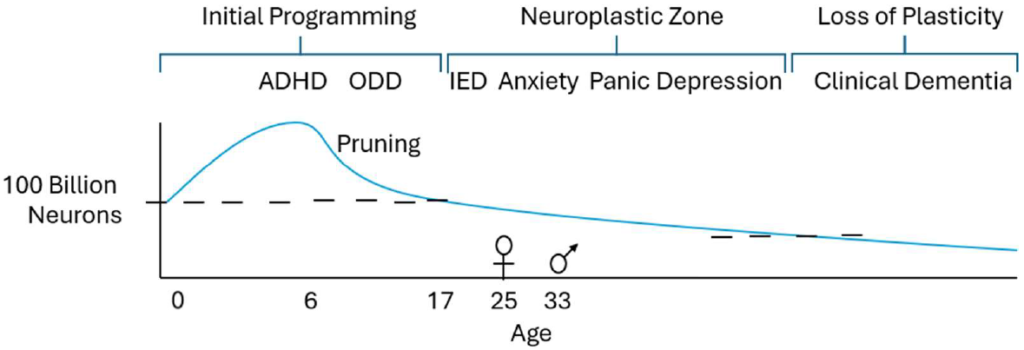
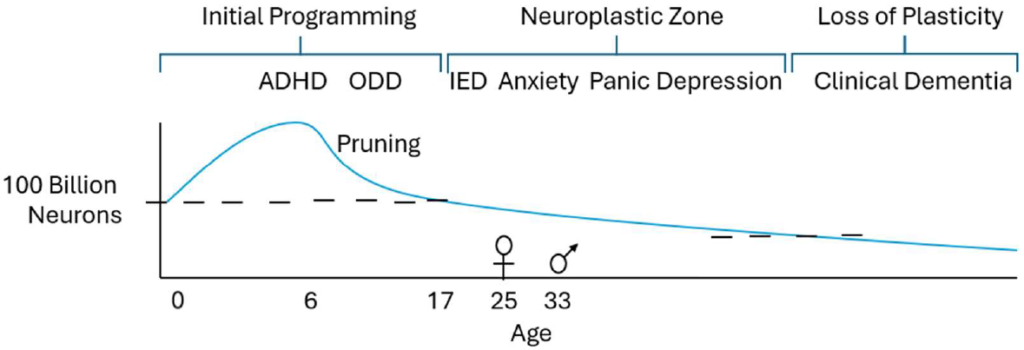
Notice the division between Oppositional Defiant Disorder (ODD) in children and Intermittent Explosive Disorder (IED) in Adults in Figure 1: Psychotherapy mirrors neurodevelopment across the lifespan. This means that the different psychotherapies that helps these psychiatric diagnoses as we age support our understanding of brain health and its misuse:
There are three overall phases in brain development when viewed from the womb to the tomb.
Initial Programming is broken into two stages: womb to age 6 and from age 6 to age 17. The first stage begins in the womb and involves the direct download of the environment into the unconscious body memory (mind) of the child. Gradually, the child learns how to approach the world through choices but faces an uphill battle to rewire the body-lessons learned in very early development. The subconscious mind is already formed. We never completely undo the early, initial programming.
The Neuroplastic Zone reflects the period of our lives when we can really learn, think for ourselves, and have the capacity to change. This ability to change our mind, form new neurons and connections, is referred to as plasticity. This plasticity is lost in the third and final phase.
Psychotherapy for the Three Neurodevelopment Phases
Initial Programming – Behavioral therapy = Parent training, Nutrition, Alpha Stim, Meditation, Meds > age 6.
Neuroplastic Zone – Psychotherapy with behavioral change sufficient to cause rewiring, Meds
Loss of Plasticity – Behavioral therapy, Meds to slow rate of neuron loss
- ADHD: primarily medication
- ODD: primarily behavioral therapy on the part of the guardians
- IED: the patient can begin to rewrite their neural wiring by repetitive behavioral change and extinguishing unhealthy dopamine-raising behaviors.
- Anxiety, panic, depression: all have great research for cognitive behavioral therapy
- Clinical dementia: and we’re back to behavioral therapy only again. Medications slow the progression of memory loss, at best, but don’t restore cognitive function once it’s lost. Detox does! Check out the supporting End of Alzheimer’s research by Dale Bredesen, M.D.
Both groups, children and elderly with dementia, rely on behavioral therapy because their executive function isn’t 100%. Thus, they are even more sensitive to neurotoxins in the water supply.
For children with Oppositional Defiant Disorder, the standard of care treatment is not medications. It is Parent-Child Interaction Therapy, which is essentially a Behavioral Therapy. It seeks to study everything that is being rewarded in the child’s life and offer perspective and modeling for how to reward the child differently. It is used in severe neurologic disorders for all ages in which the patients can’t reason with you in logical conversation. They do learn by experience, therefore Behavioral Therapy is specialized training in creating experiences for other people. Adults with IED and foster parents of severely traumatized children find out that reactions to maltreatment persist for years even if the environment is truly sound and emotionally healthy, even from electromagnetic waves, toxins in the food and water supply, restriction on the internet, no social media, a healthy support group, good sleep hygiene, access to Brene Brown resources, grounding sheets, bible study – they know it’s sometimes not enough. If you have a tough cookie, join me on a live call.
Mood Stabilizers Can Help with Intermittent Explosive Disorder
Trileptal is in an anticonvulsant, in the anti-seizure (when used for Neurology) and mood-stabilizer (when used for Psychiatry) family of medications. They work by changing the electro-potential gradient across the cell membranes of nerves all over the body through the Na+/K+ Pump by inhibiting the ATPase enzyme. The result is it takes a little stronger stimulus to get the nerve to do anything. This results in slightly slower initiation and less firing, so it can stop seizures in high enough doses. Psychiatrists often use about 1/3 the strength of the same medications to get relief of mental health symptoms, than do Neurologists to get relief for epilepsy.
- I typically start Oxcarbazepine at 300 mg by mouth twice per day on a scary, full sized adult – half of that if they’re smaller framed with not-so-scary episodes.
- I typically double it on the next visit if it’s helping only somewhat, or go up by 50% if other risk factors are present, at the follow-up appointment.
- Weight-based doses should be calculated for people around 100 pounds or less, including children. I’ve started 75 mg twice per day before.
- Note that a careful history of past violent behavior and recent trends is crucial to determining the appropriate level of psychiatric care. True tele-health is typically not an option if Trileptal and a Two-Minute Speech doesn’t work. The patient may need an intensive outpatient program that takes them away from their usual routine for at least six weeks.
I like to think mood stabilizers work by slowing down the nervous system so people with fast-conditions of the nervous system could see benefit: intermittent explosive disorder, attention deficit disorder, anxiety, OCD, panic disorder, etc.
The generic name is oxcarbazepine, which is what I practically always prescribe. I like how “Trileptal and a Two-Minute Speech” rolls off the tongue, even though I don’t actually prescribe brand name very often (working in the Army, VA, and prisons won’t allow). As a psychiatrist, I’m always noticing simpler ways to make things memorable and meaningful. Other medications I’ve sometimes used for IED in the same family are Tegretol (carbamazepine), Lamictal (lamotrigine), Lithium, Depakote (has a chance of making it worse). Keppra (levetiracetam) is often used for seizures but can worsen anger or cause secondary IED.
In summary, we have covered synaptic plasticity, treatment of Intermittent Explosive Disorder, and discussed childhood Oppositional Defiant Disorder. Trileptal and a Two-Minute speech may slow the IED brain down enough for the adult to change their behaviors sufficient for rewiring. But does it work?
My absolute favorite story of how good mental health treatment (anger management) can help stabilize vulnerable communities (Rural Alaska, pay attention)

While deployed to the Texas-Mexico border in 2022, I simultaneously pulled civilian duty as a tele-psychiatrist for 4 different private, federally-contracted prisons. During such times of stress, Intermittent Explosive Disorder was commonplace among my patients in prison, and the Soldiers and Airmen I would see on the base. I got real fast at giving the same 2-minute speech to angry Soldiers, Airmen, and prisoners (some of which were veterans). The first emotional support animal I trained to be a PTSD service dog, CPT Tigger, helped deescalate in the absence of Trileptal.
The most amazing thing happened during this busy time. I was seeing a prisoner with IED that could not stay out of trouble. Every day he was getting into fights and being put in solitary confinement. It was getting close to the end of his prison sentence and other inmates were provoking him on purpose so that he would get more time added. It was breaking his heart, which is why IED is a disorder and not sociopathy. He had been a sociopath for most of his life, but had a change of heart – something modern psychiatric diagnoses wouldn’t suggest possible. He wanted a life of freedom, only he 100% could not stop fighting when triggered. I remember he had tattoos all over his face. The world and other mental health professionals had given up on him.
I gave the prisoner Trileptal and my Two-Minute speech and then didn’t seem him again for two months. The next time I saw him, everything had changed. It was miraculous and the two counselors physically in the room with him noticed it too. He was peaceful. Not only did Trileptal and a Two-Minute Speech help him stay out of fights, but everyone was so impressed with his dramatic transformation that other prisoners began bringing their conflicts to him and he was able to de-escalate and resolve their arguments too. The effect was immediate. There were no fights from any prisoners on the entire cell block for the entire 2 months between appointments. It had been the most violent unit in the prison up until Trileptal and a Two-Minute Speech. One man decided to be bold and change his neural wiring. Remember him the next time you’re angry. Mentorship is how his gargantuan effort will live on in that story and change the world. Be blessed. May this blog post will help prevent a lot of loss and pain.
How do we make the prisons better?
- We all need to stop laughing at prison rape jokes! Consider actively protesting them.
- The climate of crime inside the prisons has to stop. Consider advocacy.
- We could simply follow Norway’s lead and institute two years of psychology in-service training to all personnel working at prisons. (Watch the documentary Norway, the Perfect Prison? Inside the World’s Toughest Prisons.) They turned their recidivism rates upside down in only one generation. Note that 20-30% of prisoners are idealogues that want to commit crimes and kill people out of their depravity, such as violent religions, cartels, and the rampant bisexual gang violence that is out there. Some simply refuse rehabilitation, but seeking the engagement of the prisoner in rehab at the outset of each prison sentence appears to recover some of the worst-of-the-worst.
- The other 70-80% are the standard recoverable folks that have typically had childhood PTSD, intermittent explosive disorder, attachment problems, mood disorders and substance abuse issues of varying duration. We can help this group and the prison guard education blight with a Scalable Intensive Outpatient Training program. I’d love to interview a prison warden that makes her employees watch these videos. We simply need corporate buy-in, instead of the abuses we’re seeing these days. They are real.
- Lobby Texas, Kansas, and New Mexico to stop allowing 18 year-olds to become ignorant prison guards because they torture prisoners with no understanding of what they are doing. Lobby Oklahoma to not reduce it’s prison guard age down to 18. Adolescents have absolutely no business in such a powerful position without any psychological education. This has a downstream effect on every fabric of society, in fact I personally believe it’s weaponized in some cases.
- Content creators and companies can provide educational materials to incarcerated individuals through programs like Edovo. I’m really interested in this and will publish a podcast if and when I start providing training on How to Mindshift directly to prisoners.